
Heart Team approach
The Heart of a Comprehensive Cardiac Surgery Program
Advanced cardiac surgery, coordinated Heart Team decision-making, cardio-kidney-metabolic prevention, and enhanced recovery—built into one integrated program.
Most major cardiovascular events do not begin on the day a patient presents. They build silently over years—through abnormal glucose, blood pressure, cholesterol, kidney dysfunction, excess adiposity, inflammation, inactivity, delayed screening, and fragmented care. Our program is designed to change that trajectory.
Begin with your baseline · Know your numbers before disease knows your body
Heart · Kidney · Metabolic
Realistic organ-level risk, layered with data and time—how silent CKM biology becomes either a prevented event or a late presentation.
Multidisciplinary Heart Team
One coordinated decision for complex disease.
A structured case conference that aligns cardiology, cardiac surgery, endocrinology, anesthesia, ICU nursing, and recovery planning around the same patient at the same time.
The burden we are designing against
Evidence, not slogans, is why a comprehensive Heart Team and ABCDES framework exist.
A program built for the full continuum of cardiac disease
This is not a narrow procedural service line. This is a comprehensive cardiac surgery program organized around early risk recognition, multidisciplinary decision-making, evidence-based intervention, perioperative optimization, enhanced recovery, and long-term prevention of recurrent disease.
We treat advanced disease.
We also work aggressively upstream.
Program pillars
Pillar 1 · Advanced Cardiac Surgery — we treat complex coronary artery disease, severe valve disease, aortic pathology, structural and multi-morbidity patients.
Pillar 2 · CKM / CRMS Prevention and Reversibility — cardiovascular, kidney, and metabolic disease managed as one connected syndrome.
Pillar 3 · Multidisciplinary Heart Team — patient-centered, guideline-aligned collective decision-making for complex disease.
Pillar 4 · ERAS Cardiac — protocolized, evidence-based optimization and recovery to improve outcomes and value-based care.
Pillar 5 · ABCDES Framework — A1C, Blood Pressure, Cholesterol, Diet, Exercise, and Screenings as an operating language for prevention.
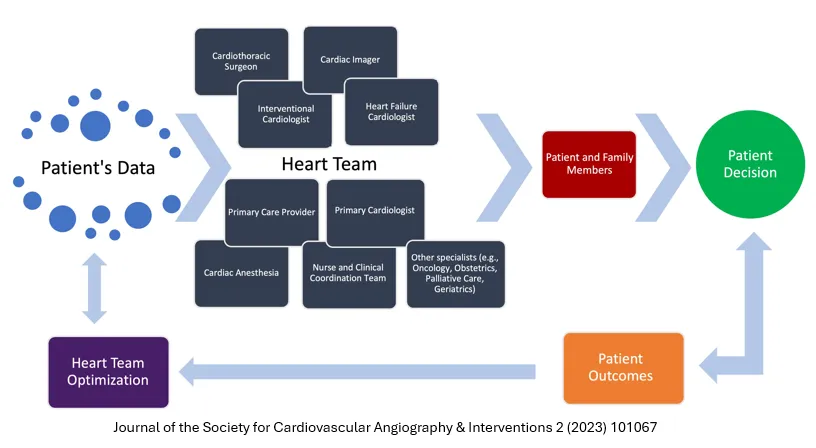
The Heart Team approach to cardiac care
Complex cardiovascular disease deserves more than a single opinion. Our program uses a multidisciplinary Heart Team model for complex coronary disease, valvular disease, aortic disease, and patients with multiple comorbidities. This model mirrors the best features of modern tumor-board style cancer care: multiple experts, one patient, one coordinated decision pathway.
The Heart Team is a patient-centered model that brings together cardiology, cardiac surgery, imaging specialists, anesthesia, critical care, nursing, endocrinology when needed, rehabilitation, care coordination, and referring physicians when appropriate. The goal is simple: determine the right treatment, for the right patient, at the right time, for the right reason.
“The Heart Team approach is guideline-endorsed in modern cardiovascular care. ACC/AHA guidance recommends multidisciplinary Heart Team decision-making when the optimal revascularization strategy is unclear, highlights the Heart Team in diabetes with multivessel coronary artery disease, and recommends multidisciplinary valve team evaluation for severe valvular heart disease being considered for intervention.”
Heart Team hub-and-spoke
Shared decision-making
The patient is not presented with a disconnected series of opinions. The patient receives an integrated recommendation.
Bias reduction
No single specialty should dominate a complex decision that has multiple legitimate pathways.
Comprehensive assessment
Anatomy, physiology, frailty, kidney function, diabetes, surgical risk, imaging findings, patient goals of care, and recovery capacity are considered together.
Outcome optimization
Better decisions improve quality, consistency, safety, short and long-term outcomes.
Two views, one coordinated pathway
The same Heart Team must make sense for patients and families and for referring physicians who trust us with complex disease.
Patient & family view-Patient at the Center Stage
You should not have to choose between conflicting recommendations. You should not have to guess which specialist is seeing the whole picture.
- One coordinated Heart Team visit instead of multiple disconnected opinions.
- Clear explanation of options, risks, and expected recovery.
- Attention to kidney function, diabetes, frailty, and long-term health—not just the procedure.
- Recovery designed through ERAS, not improvised day by day.
Referring physician view
A high-reliability, multidisciplinary cardiac surgery program built for complex disease, better decision quality, perioperative optimization, and longitudinal risk reduction.
- Rapid triage and clear Heart Team recommendations.
- Thoughtful revascularization and valve strategy discussions.
- Embedded CKM / CRMS recognition and ERAS-informed perioperative care.
- Structured communication and continuity back to the referring team.
Academic deep dive: CKM, CRMS, and the Heart Team
Toggle between the concise takeaway and the academically detailed view. The same framework must work for patients and for colleagues reading the primary literature.
Concise: CKM / CRMS frameworks recognize that cardiovascular disease, kidney disease, diabetes, obesity, and metabolic dysfunction are not separate silos. They are interconnected biology that demands integrated risk detection, prevention, and treatment. Our Heart Team uses these frameworks to shape revascularization, valve strategy, perioperative optimization, and long-term prevention.
Why we intervene before the event
Presentation is late. Biology starts early. Coronary artery disease, kidney disease, and many cancers often have a silent decade before the emergency. Our Heart Team and ABCDES framework are built to operate in that decade—not just on the day of the event.
- Identify disease before symptoms.
- Correct the major upstream drivers: A1C, blood pressure, cholesterol, adiposity, inactivity, delayed screening.
- Coordinate care across specialties instead of reacting in silos.
- Use surgery when needed, but surround it with prevention and enhanced recovery.
- Reduce the chance that preventable disease keeps recurring.
The silent decade before the event
Waiting for symptoms is often waiting too long. Screening, surveillance, and baseline measurement let us act while disease is still reversible.
What happens when the body compensates for too long
The body silently absorbs metabolic, vascular, and inflammatory stress for years. Patients often look “fine” while disease is progressing. Eventually compensation fails—and the first obvious sign may be a heart attack, stroke, heart failure, kidney failure, or cancer diagnosis.
- Coronary plaque progresses quietly until subclinical ischemia becomes an emergency.
- Kidney function declines gradually until eGFR and albuminuria cross critical thresholds.
- Small colon polyps grow silently for 10–15 years before symptoms appear.
- Uncontrolled A1C and blood pressure damage microvasculature long before the first event.
Clinical message: The crisis is late; the biology is early. Our Heart Team, CKM / CRMS frameworks, ERAS Cardiac, and ABCDES model are all designed to intervene before compensation fails.
What this means for patients
You do not have to wait for a heart attack, stroke, dialysis, or late-stage cancer diagnosis to take action.
Enhanced Recovery After Surgery (ERAS) for cardiac surgery
Recovery should be designed—not improvised. ERAS is a multidisciplinary, evidence-based perioperative platform built to reduce surgical stress, improve physiologic recovery, standardize best practices, and improve patient outcomes. ERAS has now become a major framework in cardiac surgery through formal guidelines and consensus statements.
Preoperative
Patient education, expectation setting, nutrition review, anemia optimization, frailty assessment, medication review, glycemic optimization, smoking cessation, prehabilitation when possible.
Intraoperative
Standardized anesthesia strategies, blood conservation, temperature management, opioid-sparing strategies where appropriate, hemodynamic precision, and efficient surgical teamwork.
Immediate postoperative
Early extubation pathways, multimodal analgesia, delirium prevention, glucose control, kidney protection, pulmonary hygiene.
Recovery & discharge
Early mobilization, nutrition restoration, standardized discharge criteria, home recovery instructions, rehabilitation planning, follow-up continuity.
“Our cardiac ERAS platform is grounded in evidence-based perioperative care recommendations and more recent international consensus work from ERAS Cardiac, ERAS International, and the Society of Thoracic Surgeons.”
Value-based care perspective: ERAS is not about simply moving patients out faster. It is about recovering patients better—fewer complications, better patient experience, more reliable pathways, better use of resources, and improved quality and value.
The ABCDES framework
Small actions, repeated early, change outcomes later. ABCDES is our prevention-first model for risk detection and self-correction, used by both the Heart Team and referring partners.
A = A1C — know your glucose damage status early.
B = Blood Pressure — control the silent driver of stroke and heart failure.
C = Cholesterol — treat plaque risk before the event.
D = Diet — what patients eat becomes biology.
E = Exercise — movement as therapy, not suggestion.
S = Screenings — screen before symptoms for cardiovascular, kidney, and cancer risk.
The compound effect works in both directions. Small daily neglect compounds into disease. Small daily correction compounds into protection. ABCDES is built on one central idea: measure early, correct early, repeat consistently.
Quality, recovery, and the standard we hold ourselves to
Quality is not an abstract statement. It is operational. It requires evidence-based decision pathways, Heart Team alignment, ERAS process reliability, complication prevention, coordinated discharge planning, and long-term risk modification. What gets measured gets improved in a learning culture. We participate in the STS National Database.

For patients and families
You may have been told you have a heart problem, a kidney problem, diabetes, high blood pressure, high cholesterol, or weight-related risk. These often travel together. Our program is built to look at the whole picture, not just one part of it.
Refer a patient or request Heart Team review
A simple, fast, highly professional referral pathway for complex multivessel disease, valve disease, aortic pathology, CKM / CRMS overlap, and frail or multi-comorbidity patients who need team review.
- Rapid triage with clear communication back to referring physicians.
- Heart Team review where appropriate.
- ERAS-informed perioperative planning.
- Longitudinal CKM / CRMS-aware risk reduction.
Preferred use: surgical evaluation, Heart Team review, perioperative optimization, CKM / CRMS-informed planning.
For urgent or time-sensitive cases, please call the on-call cardiac surgery or cardiology team or call 911 with symptoms of chest pain or shortness of breath.
Evidence-aware, not just marketing
Our program is grounded in contemporary CKM / CRMS science, ACC/AHA guideline-directed Heart Team use, ERAS Cardiac and ERAS International consensus statements, and CDC, WHO, and professional-society epidemiology.
Selected reference anchors
- AHA Cardiovascular-Kidney-Metabolic Health Presidential Advisory (Circulation 2023).
- Synopsis of CKM evidence and management (Circulation 2023).
- ACC/AHA/SCAI coronary revascularization guideline (JACC 2021/2022).
- ACC/AHA valvular heart disease guideline (JACC 2021).
- ERAS Cardiac and ERAS International perioperative consensus statements.
- CDC, WHO, ACS, USPSTF, and IDF epidemiology and screening guidance.